
General Considerations
The goal of therapy is to alleviate symptoms when there are no consequences. The location, severity, duration, and patient preference of the stricture should all be taken into account during the therapy process.
Treatment options for acute urine retention in urethral stricture issues include direct vision internal urethrotomy (DVIU), suprapubic cystostomy, cystoscopy, and urethral dilatation.
Therapies for urethral strictures can be broadly divided into two categories: open surgical techniques, including stricture excision and anastomosis, urethroplasty, and perineal urethrostomy, and endoscopic procedures, like urethral dilatation and internal urethrotomy. Before choosing a final intervention, the stricture’s length and exact location should be identified.
Urethral dilatation: For a long time, urethral dilation with sound and boogies was the accepted first line of treatment. Tissue stretching and stricture disruption or widening result from the insertion of urethral dilators and their sequential size increases.
Direct vision internal urethrotomy:
When performing DVIU, a transurethral incision is made at the 12 o’clock position to relieve the stricture. This allows the urethral lumen to enlarge by secondary intention. With the highest success rates, this method is used as the first line of treatment for bulbar strictures that are brief (less than 2 cm) and have not been treated previously.
The decision of whether to go straight to a urethroplasty or perform a repeat DVIU after the previous procedure recurs is up for dispute. While some doctors advise a urethroplasty as the best course of action following a recurrence, others advise trying DVIU at least once more following the initial treatment.
Intermittent self-catheterization: After first therapy, intermittent self-catheterization on a regular basis helps keep the urethral lumen open.
VIU
VIU
Urethroplasty: This procedure entails resecting or opening the stricture and replacing the strictured urethral tissue with either a flap of normal skin, graft materials such buccal mucosa or foreskin, or a direct anastomosis for short (<2 cm) bulbar strictures. With a high overall success rate of >85%, this treatment usually produces good results and can be used for prolonged strictures.
Relatively rare urethroplasty complications include chordee, neuropraxia, fistulas, incontinence, erectile dysfunction, and UTIs.
Anastomotic urethroplasty:
Stricture excision and end-to-end anastomosis are more frequently referred to as anastomotic urethroplasty. This method works best when the stricture is brief (less than 2 cm) and in the bulbar urethra, which frequently happens after a traumatic straddle-type injury.
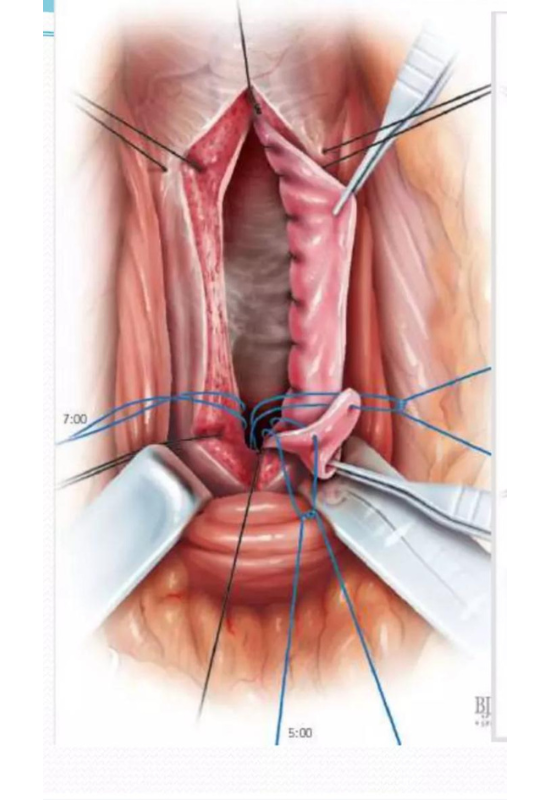
Substitution or graft urethroplasty:
Using this procedure, the urethra is mobilized in the strictured area, separated from the corpora cavernosa, and then opened longitudinally along the stricture’s length.
this procedure can be performed through a ventral, dorsal, or lateral approach. To widen the urethra, a skin graft is sutured to the defect.
The oral mucosa, foreskin, and infrequently the upper inner thigh can also be used as sources for skin grafts. Because of its histological characteristics and resilience to urine exposure, the oral mucosa makes the best transplant material.
Any penile urethral stricture or bulbar stricture too lengthy for a direct anastomotic urethroplasty should be treated with substitution urethroplasty.
For patients with complicated urethral strictures, such as those who have had lichen sclerosus, urethral reconstruction, or hypospadias treatment in the past, a two-stage procedure is advised.
 BMG URETHROPLASTY
BMG URETHROPLASTY
BMG URETHROPLASTYPerineal urethrostomy
Patients who have had numerous stricture procedures, have generally severe or difficult stricture disease, or do not want to have substantial future surgeries are the only ones eligible for this palliative procedure. Patients with numerous comorbidities who are unable to endure a urethroplasty may also benefit from perineal urethrostomy.